The Mother, Her Fight, Her Baby
Abnormalities on TIFFA scan. Fetal MRI, Amniocentesis, FISH, WES and so on .....
By Dr. Avanthi Vellala
Some cases stay with you not because of how they began, but because of how far they travelled.
She was 29. Five years of marriage. On his side OATZ. Low sperm count, low motility and poor morphology. On her side the news was harder. AMH of 0.2, follicle count of just three on each side. Numbers that, at 29, you don’t expect to hear.
I sat with them and explained everything honestly. The low success rates, the likelihood of needing multiple stimulation rounds, and the option of donor egg .
I didn’t soften it.
They heard all of it. And they said we want to try with our own.
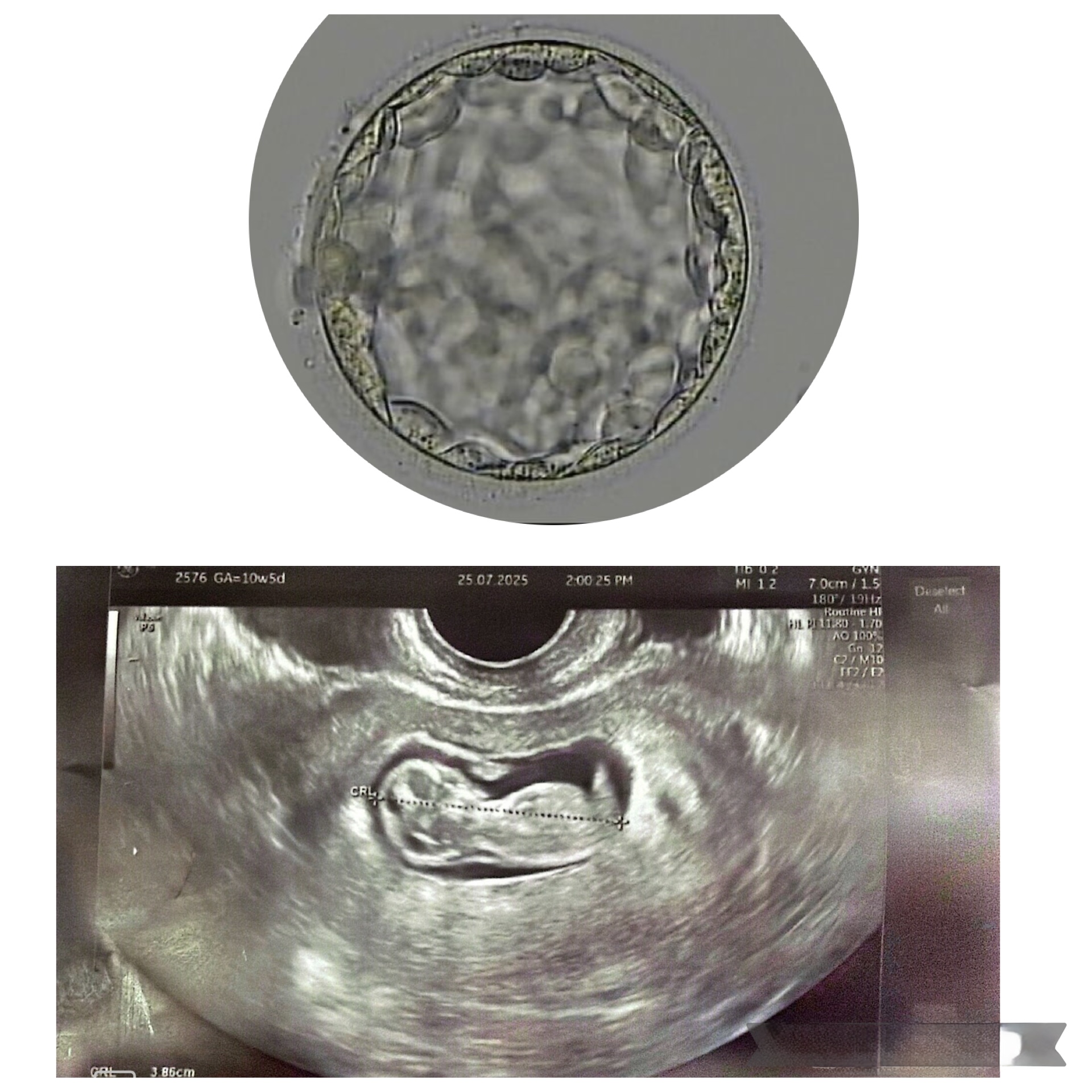
We started stimulation. I was expecting four eggs. We retrieved five. Three were mature. All three fertilised. Two made it to blastocyst.
Two blastocysts. With an AMH of 0.2 and severe male factor. That’s a remarkable response and I told them so.
We transferred one embryo. It implanted. The pregnancy progressed well.
Through every scan, every appointment, every anxious moment of that cycle her mother was beside her. Her mother who never once wavered. Every time I explained a risk or a complication, she would look at me and say the same thing “We trust you. Please do something.”
I referred her to her gynaecologist. The NT and NB scan was normal. Double marker was low risk. Everything looked fine.
And then the TIFFA scan.
The foetus was found to have bilateral ventriculomegaly and a dysgenetic corpus callosum. Two findings that changed the entire tone of the pregnancy.
A foetal MRI confirmed it bilateral ventriculomegaly with atrial diameters of 11 to 12mm, and dysgenetic corpus callosum. The corpus callosum is the bridge of nerve fibres that connects the two sides of the brain. When it doesn’t form properly, the implications can range from minimal to significant and at the time, nobody could say with certainty which direction this would go.
They went further. Amniocentesis, followed by FISH and WES Whole Exome Sequencing, which looks at the coding regions of the genome for disease causing variants.
FISH was negative for chromosomes 13, 18, 21 and the sex chromosomes.
WES showed a heterozygous missense variant in the COL1A1 gene, classified as likely pathogenic associated with Caffey disease and osteogenesis imperfecta. The minor allele frequency was 0.002%, making this an extraordinarily rare finding.
They met a paediatric neurologist. Parental testing was done. Both parents came back negative for the variant meaning this was a sporadic occurrence, not inherited.
They were referred to a geneticist. After reviewing the full picture, the geneticist advised continuing the pregnancy. The scans, apart from the ventriculomegaly and corpus callosum findings, were otherwise normal. Baby’s growth was tracking well.
At a certain point, her treating gynaecologist raised the possibility of termination not without reason. The WES finding was real, the uncertainty was real, and the medical team had a responsibility to put all options on the table.
I spoke to her.
She was determined to continue.
By the time all the reports were in, she was nearly 30 weeks. After full genetic counselling, the consensus was to continue the pregnancy with a multidisciplinary approach at delivery. Paediatricians were informed and a senior specialist was kept in the loop throughout.
She was taken for a caesarean section at 36 weeks and 3 days.
Before the section, I sent a message to the group we should do everything within our boundary to keep the mother and baby safe.
She delivered a baby boy. 2.7 kilograms. Both mother and baby fine.
Multiple tests were run on the baby. All came back normal. They were discharged.
The baby is now six months old. Doing well.
We don’t know what the future holds. Nobody can say that with certainty. But right now, everything is normal.
I want to say something about why I’m sharing this case specifically. I had another patient she conceived through IUI. Her TIFFA scan showed bowing of the legs. No genetic tests. No confirmatory workup. The pregnancy was terminated on that finding alone.
And just this morning, a patient walked into my OPD with a TIFFA report showing a prominent left ventricle. She was scared. I told her let’s do the confirmatory tests before we draw any conclusions. Her NT was normal, double marker low risk. One finding, in isolation, is not the full picture.
That’s what this case taught me or rather, reminded me. You do not jump. You follow the process. You get every test. You involve every specialist. And then you sit with the patient and you decide together.
A special word for Dr. Prithivi Perum, her treating gynaecologist. The patience, the thoroughness, the multidisciplinary coordination at every step that’s the kind of medicine that gives a mother and her baby the best possible chance.
And to this mother who knew nothing about ventriculomegaly or corpus callosum or WES variants when this journey began. Who learned everything, met every doctor, asked every question, and held on.
Her determination is the reason her baby is here.
Disclaimer: I may have missed a few details along the way this is the gist of what happened.
But I want to be honest about something that ran through my mind throughout her entire journey. If the pregnancy had been terminated, I wasn't sure what came next. We had one frozen embryo left. I didn't know if it would work. And I wasn't sure that even if we did another stimulation cycle, I could give them embryos as good as these again not with her AMH, not with his OATZ . That uncertainty stayed with me from the TIFFA scan all the way to the day she delivered.